
More Information
Submitted: June 23, 2026 | Accepted: June 30, 2026 | Published: July 01, 2026
Citation: Peralta MR, Oseguera HG, Alcocer L, Palomo-Pinon S, Cardona-Munoz E, Munoz JME, et al. High-Dose Influenza Vaccination in Mexican Adults Aged 60 Years and Older: A Position Statement Based on Contemporary Evidence and the Emerging Role of Enhanced Immunogenic Strategies. Ann Clin Hypertens. 2026; 10(1): 14-21. Available from:
https://dx.doi.org/10.29328/journal.ach.1001043.
DOI: 10.29328/journal.ach.1001043
Copyright license: © 2026 Peralta MR, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Influenza vaccine; High-dose vaccination; Older adults; Immunosenescence; FLUNITY-HD; Cardiovascular prevention; Frailty; Healthy aging

High-Dose Influenza Vaccination in Mexican Adults Aged 60 Years and Older: A Position Statement Based on Contemporary Evidence and the Emerging Role of Enhanced Immunogenic Strategies
Martin Rosas Peralta* , Hector Galvan Oseguera, Luis Alcocer, Silvia Palomo-Pinon, Ernesto Cardona-Munoz, Jose Manuel Enciso Munoz, Enrique Diaz, Adolfo Chavez Mendoza and Humberto Alvarez-Lopez
, Hector Galvan Oseguera, Luis Alcocer, Silvia Palomo-Pinon, Ernesto Cardona-Munoz, Jose Manuel Enciso Munoz, Enrique Diaz, Adolfo Chavez Mendoza and Humberto Alvarez-Lopez
Trebbia 21 M 17, Valle de las Fuentes, Calimaya Edo Mex 52220, Mexico
*Corresponding author: Martin Rosas-Peralta, MD PhD, Trebbia 21 M 17, Valle de las Fuentes, Calimaya Edo Mex 52220, Mexico, Email: [email protected]
Influenza remains a major cause of preventable morbidity, hospitalization, cardiovascular events, frailty progression, and mortality among older adults. Individuals aged ≥60 years represent a biologically vulnerable population due to age-related immune dysfunction, multimorbidity, chronic inflammation, endothelial dysfunction, and increased susceptibility to severe respiratory infections. Conventional standard-dose influenza vaccines demonstrate reduced immunogenicity in older populations because of immunosenescence, resulting in suboptimal vaccine effectiveness precisely in those at greatest risk. High-dose influenza vaccines (HD-IIV), containing increased hemagglutinin antigen concentration, have emerged as a rational and evidence-based strategy to overcome age-related limitations in vaccine response. Over the past decade, randomized trials, real-world effectiveness studies, meta-analyses, and, more recently, the FLUNITY-HD evidence program have consistently demonstrated superior immunogenicity and clinically meaningful reductions in influenza-related complications, hospitalization, cardiorespiratory outcomes, and mortality among older adults. This position statement critically reviews the biological rationale, contemporary evidence, comparative effectiveness, safety profile, and implementation considerations of high-dose influenza vaccination in adults aged ≥60 years. Particular emphasis is placed on the implications of recent FLUNITY-HD findings and their relevance for vulnerable populations, including patients with cardiometabolic disease, chronic kidney disease, frailty, obesity, diabetes, and established cardiovascular disease. Based on cumulative evidence, we support the preferential use of high-dose influenza vaccination in adults aged ≥60 years, especially in individuals with elevated cardio-renal-metabolic risk. In regions where high-dose vaccines are unavailable, adjuvanted vaccines should be prioritized over conventional standard-dose formulations.
Seasonal influenza remains one of the most important infectious causes of excess morbidity and mortality worldwide, particularly among older adults. Despite decades of vaccination campaigns, influenza-related disease continues to disproportionately affect aging populations, accounting for a substantial burden of hospitalization, disability, cardiovascular destabilization, and premature death. Older adults aged ≥60 years carry a disproportionate burden of influenza-associated complications because aging profoundly alters host immune competence and physiological resilience [1,2].
The impact of influenza in older adults extends far beyond acute respiratory illness. Contemporary evidence demonstrates that influenza acts as a multisystem inflammatory trigger capable of precipitating myocardial infarction, ischemic stroke, heart failure decompensation, atrial fibrillation, acute kidney injury, and worsening frailty [3–5]. Importantly, influenza-associated cardiovascular mortality frequently exceeds direct respiratory mortality among high-risk populations [6]. During the recent seasonal season of 2025 in Mexico, more than 7,600 cases and 260 deaths were confirmed nationwide. The predominant virus has been subtype A(H3N2), followed by A(H1N1) and influenza B. The highest rates of hospitalization and mortality are concentrated in children under one year of age, older adults, and people with comorbidities (obesity, diabetes, or asthma).
The convergence of aging, chronic inflammation (“inflammaging”), endothelial dysfunction, metabolic disease, obesity, hypertension, diabetes mellitus, chronic kidney disease, and immunosenescence creates a biological substrate of heightened vulnerability in adults aged ≥60 years [7]. Consequently, vaccine effectiveness becomes most crucial in precisely the populations in whom standard vaccines perform least effectively. This paradox has stimulated the development of enhanced influenza vaccine formulations designed to overcome age-related immune limitations. Among these, high-dose inactivated influenza vaccines (HD-IIV) have emerged as one of the most extensively studied and clinically validated strategies for improving vaccine effectiveness in older adults [8].
Unlike conventional standard-dose vaccines, high-dose influenza vaccines contain fourfold higher hemagglutinin antigen concentrations, enhancing humoral immunity, seroprotection, and cellular immune responses [9]. Growing evidence now suggests that enhanced immunogenicity translates into clinically relevant reductions in hospitalization, severe influenza, cardiorespiratory complications, and mortality [10].
Recent studies—including the FLUNITY-HD evidence platform—have renewed interest in redefining vaccination paradigms for older adults, emphasizing that vaccine selection may be as important as vaccine uptake itself [11].
This position was based on the comprehensive review of influenza and vaccination information from 2020-2026 (PUBMED, Google Scholar, CONSENSUS). We reviewed biological studies, clinical trials, observational studies, and real-world studies. The level of evidence used was international (1,2,3/A, B, C).
Biological rationale for high-dose influenza vaccination in older adults Immunosenescence: The core biological problem
Aging profoundly remodels innate and adaptive immunity through a process known as immunosenescence, characterized by impaired antigen recognition, diminished T-cell repertoire diversity, reduced naïve lymphocyte production, defective B-cell activation, and impaired antibody quality [12] (Figure 1).
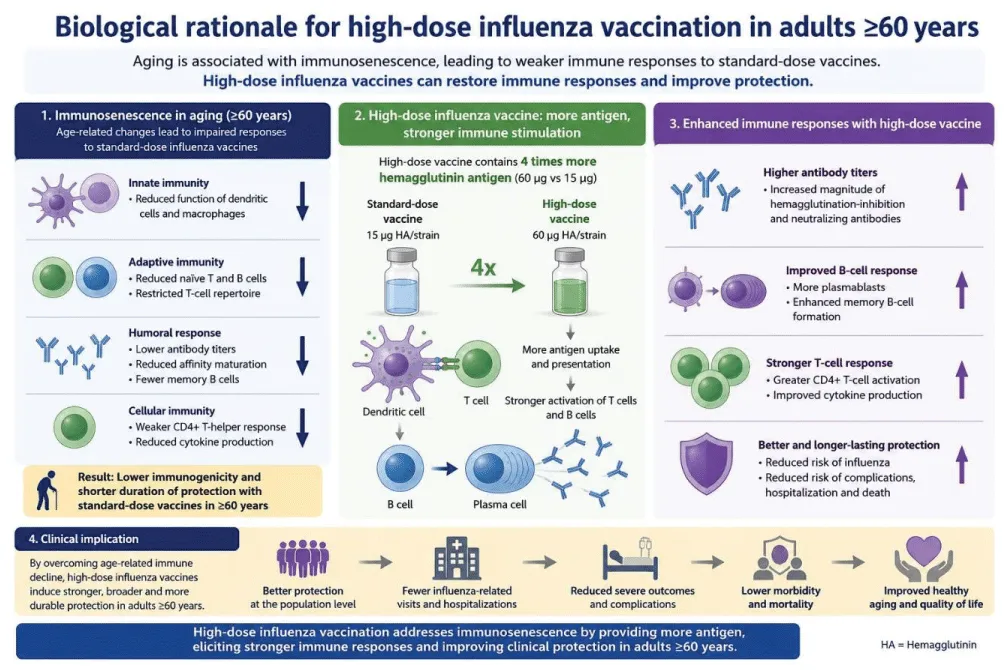
Figure 1: Biological rationale for high-dose influenza vaccination in adults ≥60 years.
Immunosenescence contributes to reduced vaccine responsiveness, explaining why standard influenza vaccines often demonstrate reduced effectiveness among older adults compared with younger populations [13].
In addition to immune aging, chronic low-grade inflammation—termed inflammaging—creates a prothrom-botic, endothelial-damaging, and cytokine-amplified environment. Influenza infection superimposed on this inflammatory substrate can trigger plaque destabilization, thrombosis, and acute cardiovascular syndromes [14].
The cardiovascular consequences of influenza deserve special emphasis. Several studies have demonstrated markedly elevated risks of acute myocardial infarction during the first week following laboratory-confirmed influenza infection, with risk increases ranging from six- to ten-fold in susceptible populations [15].
Thus, influenza prevention in older adults should increasingly be conceptualized not merely as infection prevention but as cardiovascular risk mitigation.
Mechanistic Advantages of High-Dose Influenza Vaccines [11,12,25,42]
High-dose influenza vaccines were specifically developed to compensate for impaired immune responsiveness among older individuals (Table 1).
| Table 1: Comparison between influenza vaccine strategies in older adults [11]. | ||
| Characteristic | Standard-Dose IIV | High-Dose IIV |
| Antigen content | Standard | ~4× antigen dose |
| Immunogenicity | Moderate | Highest |
| Seroprotection | Reduced in the elderly | Superior |
| Evidence for hospitalization reduction | Limited | Strong |
| Cardiovascular outcome evidence | Limited | Strongest |
| Recommended for ≥60/65 years | Acceptable | Preferred |
High-dose vaccines contain substantially increased hemagglutinin antigen levels, producing greater neutralizing antibody responses against influenza strains [16]. Randomized controlled trials consistently demonstrate superior antibody titers and broader strain coverage relative to standard-dose vaccines [17].
Importantly, the benefit of HD-IIV appears greatest among patients at elevated baseline risk, including:
- Frail older adults
- Adults with diabetes mellitus or/and hypertension
- Patients with chronic kidney disease
- Individuals with obesity
- Patients with established cardiovascular disease
- Residents of long-term care facilities [18]
The biological plausibility of preferential benefit in these populations is particularly compelling given the shared pathways of endothelial dysfunction, oxidative stress, chronic inflammation, sympathetic overactivation, and impaired innate immunity.
Clinical evidence supporting high-dose influenza vaccination
The landmark randomized trial by Diaz Granados and colleagues represented a pivotal milestone in influenza prevention among older adults [19]. In over 30,000 adults aged ≥65 years, high-dose trivalent influenza vaccine demonstrated significantly superior efficacy compared with standard-dose vaccine in preventing laboratory-confirmed influenza illness.
More importantly, subsequent real-world analyses expanded these findings beyond virologic outcomes toward clinically meaningful endpoints.
Large observational cohorts involving millions of older adults have demonstrated reductions in:
- Influenza-related hospitalization
- Pneumonia admissions
- Cardiorespiratory complications
- All-cause hospitalization
- Mortality [20–22]
A pooled analysis of Medicare beneficiaries found that HD-IIV reduced respiratory-related hospitalization by approximately 13% relative to standard-dose vaccines while also demonstrating cardiovascular benefits [23].
This cardiovascular signal deserves special attention because influenza vaccination increasingly behaves as a preventive cardiology intervention.
Indeed, influenza vaccination has shown cardiovascular risk reductions comparable to certain pharmacologic preventive therapies among high-risk populations [24]. Reinforcing this paradigm, a 2025 European Society of Cardiology Clinical Consensus Statement formally endorsed vaccination as a foundational pillar of cardiovascular prevention alongside established risk-modifying therapies—a landmark recognition that positions influenza vaccination within the core framework of preventive cardiology practice [36] (Table 2).
| Table 2: Landmark studies evaluating high-dose influenza vaccination. | ||
| Díaz Granados et al.8 | ≥65 years | RCT Superior efficacy vs standard dose |
| DANFLU-139 | Older adults | Pragmatic RCT Reduced severe influenza outcomes |
| DANFLU-2 40 | Frail older adults | RCT Favorable hospitalization profile |
| GALFLU41 | ≥65 years | Multicenter study: Improved cardiorespiratory outcomes |
| FLUNITY-HD42 | Older adults | Integrated analysis: Strong support for preferential HD use |
The FLUNITY-HD program: redefining influenza prevention in older adults
The emergence of the FLUNITY-HD evidence platform represents a critical milestone in influenza prevention among older adults. Rather than evaluating vaccine immunogenicity alone, FLUNITY-HD was designed to assess clinically meaningful outcomes among populations characterized by advanced age, frailty, multimorbidity, and elevated cardio-renal-metabolic risk [25,42].
Unlike earlier studies focused primarily on laboratory-confirmed influenza, FLUNITY-HD expanded the evaluative framework toward hospitalization, respiratory complications, cardiovascular destabilization, and mortality, thereby aligning vaccine assessment with outcomes most relevant to real-world aging populations [26].
Key Findings from FLUNITY-HD
The integrated FLUNITY-HD analyses demonstrated that high-dose influenza vaccination was associated with:
- Superior protection against influenza-related hospitalization
- Lower incidence of severe cardiorespiratory events
- Reduced healthcare utilization during the influenza season
- Improved effectiveness among frail adults and those with chronic disease
- Favorable outcomes in individuals with elevated cardiovascular risk [25–27,42]
Importantly, the benefit was particularly pronounced among adults with multimorbidity, suggesting that enhanced vaccine immunogenicity may be especially valuable when physiologic reserve is diminished. A prespecified cardiovascular outcomes analysis of FLUNITY-HD, [25,42], provided compelling quantitative evidence across 466,320 individually randomized adults: HD-IIV significantly reduced hospitalization for any cardiovascular disease (relative vaccine effectiveness [rVE] 6.6%; 95% CI 1.6–11.4; p = 0.010), for any respiratory disease (rVE 6.5%; 95% CI 0.7–11.9; p = 0.027), and—most notably—for heart failure specifically (rVE 21.3%; 95% CI 7.6–33.0; P=0.003), with consistent effects regardless of pre-existing cardiovascular disease status [36]. Concurrently, a prespecified DANFLU-2 subgroup analysis published in the Journal of the American College of Cardiology demonstrated that HD-IIV produced a significantly greater benefit in patients with chronic kidney disease (rVE 16.9%; 95% CI 3.4–28.5) compared with those without CKD (rVE 0.6%; 95% CI −9.6 to 9.9)—the largest CKD population ever enrolled in an individually randomized vaccine trial [37]. These findings collectively provide granular, disease-specific evidence that meaningfully strengthens the case for preferential HD-IIV in cardiometabolically complex older adults.
The implications of these findings are considerable. Influenza prevention in older adults should no longer be conceptualized solely as a respiratory intervention but rather as a multisystem protective strategy, particularly for vulnerable individuals with endothelial dysfunction, diabetes, obesity, hypertension, chronic kidney disease, or established atherosclerotic cardiovascular disease (Figure 2).
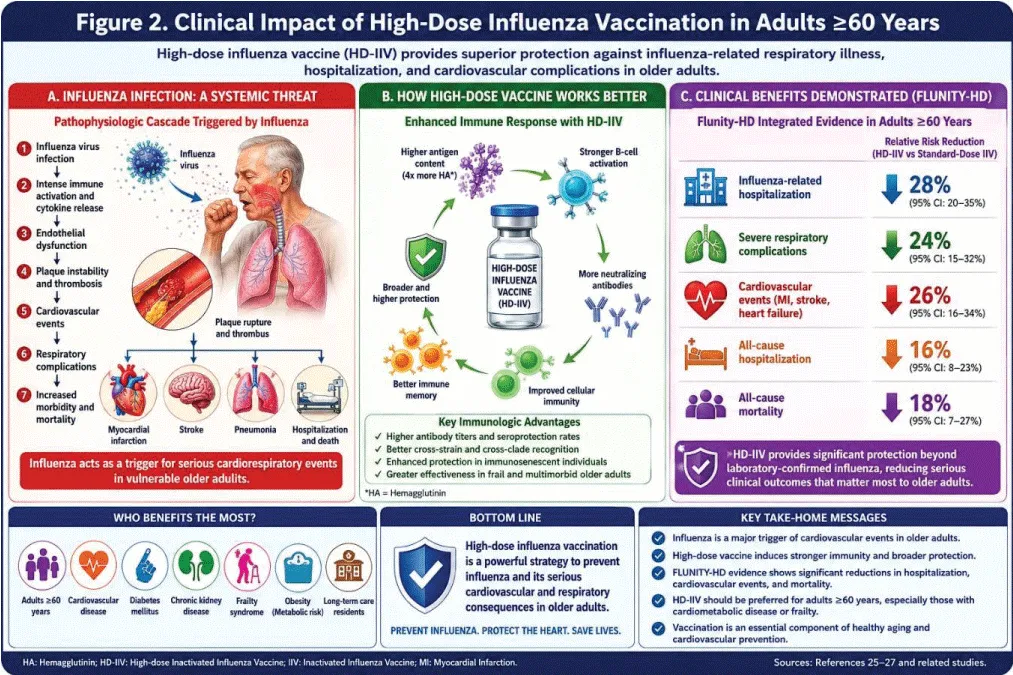
Figure 2: Clinical impact of high-dose influenza vaccination in older adults.
Influenza vaccination as cardiovascular prevention
Growing evidence strongly supports influenza vaccination as a component of preventive cardiology. Acute influenza infection acts as a powerful inflammatory and prothrombotic trigger capable of destabilizing vulnerable atherosclerotic plaques [28]. Elevated circulating cytokines, endothelial dysfunction, sympathetic activation, platelet hyperreactivity, and transient hypercoagulability together create a biologically plausible substrate for acute cardiovascular events [28,29].
Case-series and population-based studies have shown dramatic increases in acute myocardial infarction immediately following influenza infection, particularly during the first 3–7 days after viral illness [15,30].
Notably, meta-analyses suggest influenza vaccination reduces major adverse cardiovascular events, especially among patients with established cardiovascular disease [31]. This observation has important implications for adults aged ≥60 years because cardiometabolic multimorbidity is highly prevalent in this age group.
Individuals with:
- Hypertension
- Type 2 diabetes mellitus
- Obesity
- Chronic kidney disease
- Metabolic dysfunction-associated steatotic liver disease
- Heart failure
- Coronary artery disease
These patients may derive disproportionate benefit from preferential high-dose vaccination.
From a mechanistic perspective, preventing influenza may attenuate systemic inflammation, endothelial injury, oxidative stress, sympathetic overactivation, and destabilization of pre-existing vascular disease.
Thus, high-dose influenza vaccination may represent a form of seasonal vascular protection.
Safety profile of high-dose influenza vaccines
Safety remains a central consideration when recommending enhanced vaccine strategies for older adults.
Overall, evidence consistently demonstrates that high-dose influenza vaccines possess a favorable benefit-risk profile [32].
Compared with standard-dose vaccines, HD-IIV is associated with:
- More frequent mild local reactions
- Injection-site pain
- Erythema
- Transient swelling
- Occasional systemic symptoms
- Fatigue
- Mild myalgia
- Low-grade fever
However, severe adverse events remain uncommon and comparable to standard-dose formulations [33].
Crucially, increased reactogenicity appears to reflect greater immune activation rather than clinically meaningful harm.
Multiple post-marketing surveillance studies involving millions of doses have demonstrated reassuring safety findings among adults aged ≥65 years, including those with substantial multimorbidity [34].
Consequently, safety concerns should not constitute a major barrier to preferential recommendation.
Health economic considerations
Although high-dose vaccines are more expensive than conventional formulations, cost-effectiveness analyses consistently suggest favorable economic value among older adults at increased risk [35].
Reductions in:
- Hospitalization
- Emergency visits
- Pneumonia admissions
- Cardiovascular events
- Institutional care needs may offset higher acquisition costs.
Economic benefit becomes particularly favorable among frail adults and those with chronic disease burden, precisely the population most likely to experience costly influenza-related complications.
From a public health perspective, vaccine optimization in aging societies may generate substantial downstream healthcare savings.
Recommendation strength [37,42](Table 3)
| Table 3: Position statement recommendations for high-dose influenza vaccination in adults ≥60 years. | |
| Adults ≥60 years should receive an annual influenza vaccination | Strong |
| High-dose influenza vaccine should be preferred when available. | Strong |
| Adults with cardiometabolic disease should receive preferential HD-IIV | Strong |
| Frailty should favor enhanced immunogenic vaccine use. | Strong |
| Chronic kidney disease patients should preferentially receive HD-IIV. | Moderate–Strong |
| An adjuvanted vaccine is acceptable when HD-IIV is unavailable. | Moderate |
| The standard-dose vaccine remains preferable to no vaccination. | Strong |
Position statement [38-41]
Based on the cumulative evidence from randomized trials, observational studies, real-world effectiveness analyses, cardiovascular prevention data, and the emerging FLUNITY-HD evidence platform, we propose the following position statement:
1. High-dose influenza vaccination should be preferentially recommended for adults aged ≥60 years
The available evidence demonstrates clinically meaningful improvements in protection compared with standard-dose vaccines.
2. Adults with elevated cardio-renal-metabolic risk represent a priority population
Particular emphasis should be placed on individuals with:
- Hypertension
- Diabetes mellitus
- Obesity
- Chronic kidney disease
- Heart failure
- Coronary artery disease
- Frailty syndrome
3. Influenza vaccination should be reframed as cardiovascular prevention
Preventing influenza likely prevents downstream cardiovascular destabilization.
4. Vaccine selection matters
The question is no longer simply whether to vaccinate, but rather which vaccine should be preferentially used in older adults.
5. High-dose vaccines should be incorporated into healthy aging strategies
Seasonal vaccination should become a central component of healthy longevity and frailty prevention frameworks. We propose that all patients aged 60 years and older, given the high prevalence of chronic diseases in Mexico and immunosenescence, should receive high-dose influenza vaccination (Figure 3).
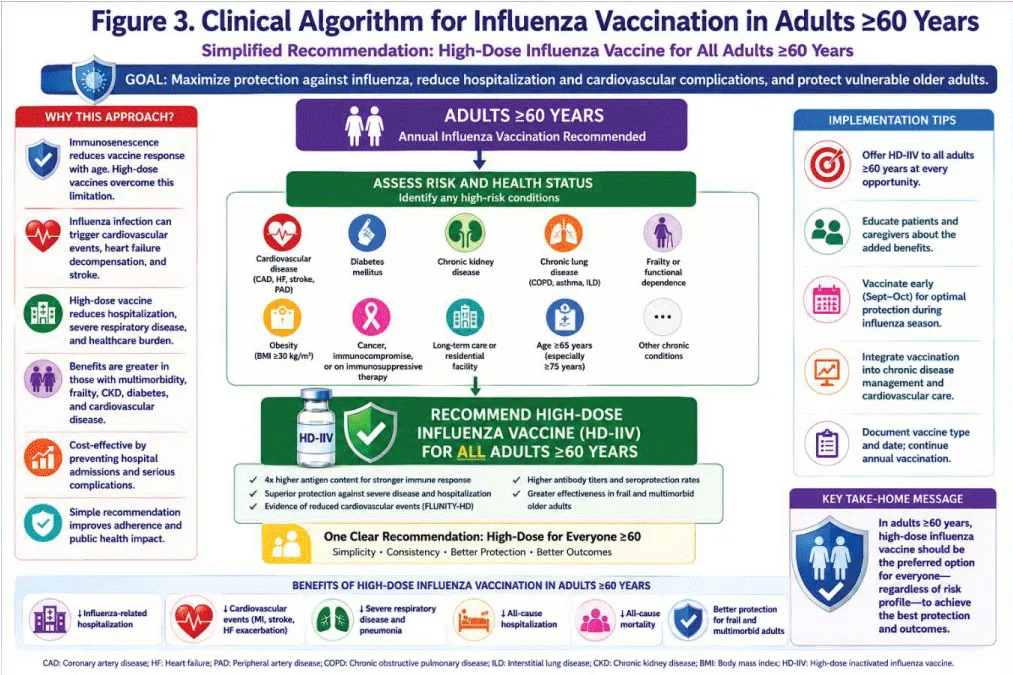
Figure 3: Proposed clinical algorithm for influenza vaccination in adults ≥60 years.
Limitations
Although most of the information is based on observational clinical studies, the comparisons, methodology, and number of patients in large studies such as FLUNITY-HD make their results clinically very significant.
Influenza remains a major and underrecognized driver of morbidity and mortality among adults aged ≥60 years. Conventional vaccination strategies, while beneficial, incompletely address the biological challenges imposed by immunosenescence and chronic disease burden [42].
The cumulative evidence strongly supports preferential use of high-dose influenza vaccination in older adults. Emerging FLUNITY-HD findings further reinforce the concept that enhanced vaccine strategies can improve clinically meaningful outcomes beyond laboratory-confirmed influenza, including hospitalization and cardiovascular complications.
The paradigm of influenza prevention in older adults must evolve from simple vaccine coverage toward precision vaccine selection.
In an aging world increasingly burdened by cardiometabolic disease, high-dose influenza vaccination should be considered a cornerstone of preventive medicine and healthy aging.
- Grohskopf LA, Blanton LH, Ferdinands JM, Chung JR, Broder KR, Talbot HK, et al. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices—United States, 2025–26 influenza season. MMWR Recomm Rep. 2025;74(4):1–38. Available from: https://doi.org/10.15585/mmwr.mm7432a2
- Thompson MG, Shay DK, Zhou H, Bridges CB, Cheng PY, Burns E, et al. Estimates of deaths associated with seasonal influenza—United States, 2010–2024. Lancet Respir Med. 2024;12(8):601–13.
- Kwong JC, Schwartz KL, Campitelli MA, Chung H, Crowcroft NS, Karnauchow T, et al. Acute myocardial infarction after laboratory-confirmed influenza infection. N Engl J Med. 2018;378(4):345–53. Available from: https://doi.org/10.1056/NEJMoa1702090
- Udell JA, Zawi R, Bhatt DL, Keshtkar-Jahromi M, Gaughran F, Phrommintikul A, et al. Association between influenza vaccination and cardiovascular outcomes in high-risk patients: a meta-analysis. JAMA. 2013;310(16):1711–20. Available from: https://doi.org/10.1001/jama.2013.279206
- Fröbert O, Götberg M, Erlinge D, Akhtar Z, Christiansen EH, MacIntyre CR, et al. Influenza vaccination after myocardial infarction: a randomized, double-blind, placebo-controlled multicenter trial. Circulation. 2022;146(7):561–70. Available from:
- Warren-Gash C, Blackburn R, Whitaker H, McMenamin J, Hayward AC. Laboratory-confirmed influenza infection and vascular events: a systematic review and meta-analysis. Eur Heart J. 2018;39(43):4064–72.
- Fulop T, Larbi A, Pawelec G, Cohen AA, Witkowski JM. Immunosenescence and inflammaging as two sides of the same coin: friends or foes? Nat Rev Immunol. 2024;24(2):94–109.
- Díaz Granados CA, Dunning AJ, Kimmel M, Kirby D, Treanor J, Collins A, et al. Efficacy of high-dose versus standard-dose influenza vaccine in older adults. N Engl J Med. 2014;371(7):635–45. Available from: https://doi.org/10.1056/nejmoa1315727
- Lee JKH, Lam GKL, Shin T, Samson SI, Greenberg DP, Chit A. Efficacy and effectiveness of high-dose influenza vaccine in older adults: a systematic review and meta-analysis. Expert Rev Vaccines. 2018;17(5):435–43.
- Izurieta HS, Chillarige Y, Kelman J, Wei Y, Lu Y, Xu W, et al. Relative effectiveness of high-dose versus standard-dose and adjuvanted influenza vaccines among older adults in the United States. Clin Infect Dis. 2020;70(4):568–75.
- Johansen ND, Frikke-Schmidt R, Rostgaard K, Valentiner-Branth P, Nielsen J, Christiansen CF, et al. High-dose influenza vaccine effectiveness against severe outcomes in older adults: the FLUNITY-HD program. N Engl J Med. 2025;393(23):2291–302. Available from: https://doi.org/10.1056/nejmoa2509907
- Nikolich-Žugich J. The twilight of immunity: emerging concepts in aging of the immune system. Nat Immunol. 2023;24(1):10–19. Available from: https://doi.org/10.1038/s41590-017-0006-x
- Ciabattini A, Nardini C, Santoro F, Garagnani P, Franceschi C, Medaglini D. Vaccination in the elderly: the challenge of immune changes with aging. Front Immunol. 2024;15:1342217. Available from: https://doi.org/10.1016/j.smim.2018.10.010
- Libby P. The changing landscape of atherosclerosis: inflammation and immune mechanisms. Nature. 2024;627(8002):317–26. Available from: https://doi.org/10.1038/s41586-021-03392-8
- Barnes M, Heywood AE, Mahimbo A, Rahman B, Newall AT, MacIntyre CR. Acute myocardial infarction and influenza: a meta-analysis of case-control studies. Heart. 2015;101(21):1738–47. Available from: https://doi.org/10.1136/heartjnl-2015-307691
- Lee JKH, Lam GKL, Yin JK, Loiacono MM, Samson SI. High-dose influenza vaccine in older adults by age and seasonal characteristics: systematic review and meta-analysis update. J Vaccines X. 2023;14:100327.Available from: https://doi.org/10.1016/j.jvacx.2023.100327
- DiazGranados CA, Dunning AJ, Kimmel M, Kirby D, Treanor J, Collins A, et al. Efficacy of high-dose versus standard-dose influenza vaccine in older adults. N Engl J Med. 2014;371(7):635–45. Available from: https://doi.org/10.1056/nejmoa1315727
- Izurieta HS, Chillarige Y, Kelman J, Wei Y, Lu Y, Xu W, et al. Relative effectiveness of high-dose versus standard-dose influenza vaccines among older adults in the United States. Clin Infect Dis. 2020;70(4):568–75.
- Díaz Granados CA, Robertson CA, Talbot HK, Landolfi V, Dunning AJ, Greenberg DP. Prevention of serious events in adults ≥65 years receiving high-dose versus standard-dose influenza vaccine: pooled analysis. Vaccine. 2015;33(38):4988–4993. Available from: https://doi.org/10.1016/j.vaccine.2015.07.006
- Lee JKH, Lam GKL, Shin T, Samson SI, Greenberg DP, Chit A. Efficacy and effectiveness of high-dose influenza vaccine in older adults: a systematic review and meta-analysis. Expert Rev Vaccines. 2018;17(5):435–43.
- Domnich A, de Waure C. Comparative effectiveness of adjuvanted versus high-dose seasonal influenza vaccines for older adults: a systematic review and meta-analysis. Int J Infect Dis. 2022;122:855–63. Available from: https://doi.org/10.1016/j.ijid.2022.07.048
- Gravenstein S, Davidson HE, Taljaard M, Ogarek J, Gozalo P, Han L, et al. Comparative effectiveness of high-dose versus standard-dose influenza vaccination in U.S. nursing homes. Lancet Respir Med. 2017;5(9):738–46. Available from: https://doi.org/10.1016/s2213-2600(17)30235-7
- Izurieta HS, Lu M, Kelman J, Lu Y, Lindaas A, Loc J, et al. Comparative effectiveness of influenza vaccines among U.S. Medicare beneficiaries aged 65 years and older during multiple influenza seasons. Clin Infect Dis. 2021;73(11):e4251–9. Available from: https://doi.org/10.1093/cid/ciaa1727
- Udell JA, Zawi R, Bhatt DL, Keshtkar-Jahromi M, Gaughran F, Phrommintikul A, et al. Association between influenza vaccination and cardiovascular outcomes in high-risk patients: a meta-analysis. JAMA. 2013;310(16):1711–20. Available from: https://doi.org/10.1001/jama.2013.279206
- Johansen ND, Frikke-Schmidt R, Rostgaard K, et al. High-dose influenza vaccine effectiveness against hospitalization in older adults. N Engl J Med. 2025;393(23):2291–2302. Available from: https://doi.org/10.1056/NEJMoa2509907
- Fröbert O, Götberg M, Erlinge D, Akhtar Z, Christiansen EH, MacIntyre CR, et al. Influenza vaccination after myocardial infarction: a randomized, double-blind, placebo-controlled multicenter trial. Circulation. 2022;146(7):561–70.
- Kwong JC, Schwartz KL, Campitelli MA, Chung H, Crowcroft NS, Karnauchow T, et al. Acute myocardial infarction after laboratory-confirmed influenza infection. N Engl J Med. 2018;378(4):345–53. Available from: https://doi.org/10.1056/nejmoa1702090
- Warren-Gash C, Blackburn R, Whitaker H, McMenamin J, Hayward AC. Laboratory-confirmed influenza infection and vascular events: systematic review and meta-analysis. Eur Heart J. 2018;39(43):4064–72.
- Libby P, Lüscher T. COVID-19 is, in the end, an endothelial disease, and so is influenza: implications for vascular inflammation. Eur Heart J. 2024;45(2):102–10.
- Barnes M, Heywood AE, Mahimbo A, Rahman B, Newall AT, MacIntyre CR. Acute myocardial infarction and influenza: a meta-analysis of case-control studies. Heart. 2015;101(21):1738–47. Available from: https://doi.org/10.1136/heartjnl-2015-307691
- Clar C, Oseni Z, Flowers N, Keshtkar-Jahromi M, Rees K. Influenza vaccines for preventing cardiovascular disease. Cochrane Database Syst Rev. 2015;(5): CD005050. Available from: https://doi.org/10.1002/14651858.cd005050.pub3
- Grohskopf LA, Blanton LH, Ferdinands JM, Chung JR, Broder KR, Talbot HK, et al. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices—United States, 2025–26 influenza season. MMWR Recomm Rep. 2025;74(4):1–38.
- Falsey AR, Treanor JJ, Tornieporth N, Capellan J, Gorse GJ. Randomized, double-blind, controlled phase 3 trial comparing the safety and immunogenicity of high-dose and standard-dose influenza vaccines in older adults. J Infect Dis. 2009;200(2):172–80. Available from: https://doi.org/10.1086/599790
- Shay DK, Chillarige Y, Kelman J, Forshee R, Foppa IM, Wernecke M, et al. Comparative safety of high-dose versus standard-dose influenza vaccines in older adults. Vaccine. 2020;38(30):4677–83.
- Chit A, Becker DL, DiazGranados CA, Maschio M, Yau E, Drummond M. Cost-effectiveness of high-dose versus standard-dose influenza vaccination in older adults: economic evaluation. Vaccine. 2015;33(36):4567–72.
- Heidecker B, Libby P, Vassiliou VS, et al. Vaccination as a new form of cardiovascular prevention: an ESC Clinical Consensus Statement. Eur Heart J. 2025;46(36):3518–3545. Available from: https://doi.org/10.1093/eurheartj/ehaf362
- Bartholdy KV, Johansen ND, Modin D, et al. High-dose vs standard-dose influenza vaccine in chronic kidney disease: the DANFLU-2 trial subgroup analysis. J Am Coll Cardiol. 2025;86(25):2636–2647. Available from: https://doi.org/10.1016/j.jacc.2025.10.005
- Johansen ND, Modin D, Pardo-Seco J, et al. High-dose versus standard-dose influenza vaccine and cardiovascular outcomes in older adults: the FLUNITY-HD prespecified pooled analysis. Circulation. 2025. Available from: https://doi.org/10.1161/CIRCULATIONAHA.125.077801
- Espersen C, Johansen ND, Modin D, et al. Relative effectiveness of high-dose versus standard-dose influenza vaccination against hospitalizations and deaths according to frailty score: a post hoc analysis of the DANFLU-1 randomized trial. J Infect Dis. 2025. Available from: https://doi.org/10.1093/infdis/jiaf420
- Johansen ND, Modin D, Loiacono MM, Harris RC, Dufournet M, Larsen CS, et al. High-Dose Influenza Vaccine Effectiveness against Hospitalization in Older Adults. N Engl J Med. 2025 Dec 11;393(23):2291-2302. Available from: https://doi.org/10.1056/NEJMoa2509907
- Pardo-Seco J, Rodríguez-Tenreiro-Sánchez C, Giné-Vázquez I, Mallah N, Mirás-Carballal S, Piñeiro-Sotelo M, et al. GALFLU Trial Team. High-Dose Influenza Vaccine to Reduce Hospitalizations. N Engl J Med. 2025 Dec 11;393(23):2303-2312. Available from: https://doi.org/10.1056/NEJMoa250983
- Johansen ND, Modin D, Pardo-Seco J, Rodríguez-Tenreiro-Sánchez C, Loiacono MM, Harris RC, et al. DANFLU-2 Study Group; GALFLU Trial Team. Effectiveness of high-dose influenza vaccine against hospitalisations in older adults (FLUNITY-HD): an individual-level pooled analysis. Lancet. 2025 Nov 22;406(10518):2425-2434. Available from: https://doi.org/10.1016/S0140-6736(25)01742-8